
Morton's Neuroma Causes
Common Causes
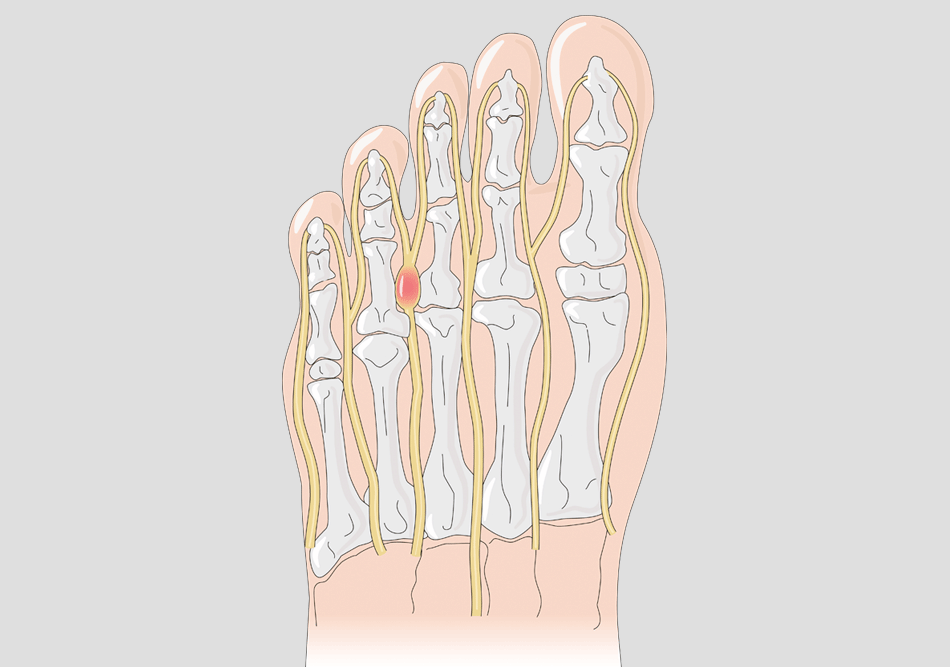
Morton’s neuroma develops when repeated pressure and shear irritate the small nerve between the toes (most often between the third and fourth). Contributing factors usually fall into four groups:
- Biomechanical: excess forefoot loading from over-pronation, reduced big-toe function, tight calf muscles, or altered gait.
- Anatomical: bunion-related toe crowding, hammertoes/clawing, a long second or third metatarsal, or a naturally splayed forefoot.
- Activity & sport: repetitive forefoot impact or compression—common in ballet/dance, football, cycling (stiff shoes), and skiing (tight boots).
- Footwear: high heels, tapered/narrow toe boxes, stiff or poorly cushioned soles.
The condition is diagnosed more often in women, likely reflecting footwear and toe-box compression; however, it can affect anyone. Dancers are particularly prone, and we have experience supporting young performers.

Biomechanical Causes
In order to manage Morton’s neuroma, it’s important that we understand and treat the mechanical factors that lead to the condition.
Some people can wear high-heeled shoes all day without ever suffering from a neuroma. Others develop the condition whilst hardly ever wearing such footwear. So why is this?
The explanation lies in understanding the structure of the foot through biomechanics and gait analysis. This is why we offer highly advanced gait (walking and running) assessments in our dedicated 3D gait laboratory – one of the most advanced of its kind anywhere in the world today.
A number of treatments, such as injection therapy and cryosurgery, can address the symptoms of Morton’s neuroma. But if the underlying biomechanical cause is not addressed, there is a greater risk that the condition will recur. Morton's neuroma also often develops because of abnormal biomechanical stress through the foot. This can lead to other conditions such as bursitis and arthritis. These in-depth biomechanical and gait assessments can sometimes avoid the need for surgery altogether and prevent the condition from recurring. Examples of the many possible biomechanical causes of neuromas and interdigital nerve irritation include:
There are many reasons why the first metatarsal can become unstable. These include abnormal pronation (where the foot arch drops and the ankle collapses excessively when walking or running), bunions, hallux limitus (a stiff big toe joint) and foot hypermobility (double-jointedness).
With an unstable metatarsal, not enough pressure passes through the joint of the big toe. This overloads the adjacent metatarsals and can result in a neuroma forming.
As part of our gait analysis service, we use an advanced method of measuring in-shoe pressure to detect this type of overload. Changing these pressures so they fall within a normal range is a key part of the treatment we can provide.
Lesser toes (i.e. all toes other than the big toe) can retract due to various and often inherited causes, such as a foot with reduced upward ankle motion (‘ankle equinus’). In this case, the ‘fat pad’ under the ball of the foot moves and the forefoot becomes overloaded, which causes a neuroma to form.
In other cases, underlying conditions such as rheumatoid arthritis may cause the fat pad to move. Specific types of orthoses can encourage the fat pad to sit back under the ball of the foot.
Various abnormalities elsewhere in the body can cause excessive stress on the forefoot, resulting in a neuroma. For example, having legs of different lengths will create greater force on one side over the other.
A difference in leg lengths can also provoke back pain and sciatica, which in turn can agitate the nerves between the toes. A change in the position of the hip, knee or pelvis will alter the way the foot interacts with the ground, which often causes metatarsal instability.
Abnormal pronation occurs when the foot arch remains flat for too long and the ankle collapses into a position, known as ‘eversion’. Typically this results in bulging at the inside of the ankle.
Using our 3D analysis system we can measure such movement very accurately (see an image of our 3D multi-segmental analysis to the right).
We also provide advanced kinetic techniques using our pressure measuring technology to further assess foot function.
Abnormal pronation, which causes the forefoot to become unstable, together with excessive metatarsal movement can provoke a shearing stress on the nerve and lead to the formation of a neuroma.
Specially designed orthoses can help with pronation issues and deal with Morton’s neuroma symptoms. Just as not all reading glasses are the same, the design and sophistication of orthoses vary according to a patient’s needs and the manufacturing method. For this reason, we may still recommend that a patient tries orthoses if they have previously used models that we consider to be inappropriate.
Anatomical Causes
Several studies have shown that people whose metatarsals are situated close together are more likely to develop Morton's neuroma. In these cases, the neuroma may be more likely to recur after treatment. It may also be more resistant to conservative treatments like orthoses.
Some people are more "bony" and lack natural padding under their feet. For others, the fat pad may have wasted away because of multiple steroid injections (which is why we discourage multiple injections).
For people who have these characteristics and suffer from Morton’s neuroma, the main treatment is to reduce focal force to a more normal level. This is measured with our kinetic pressure system, and treatment comes in the form of prescription orthoses and footwear change.
Whilst there are also various "fillers" that can be injected under the ball of the foot, we do not endorse this procedure. This is because most "dermal fillers" break down and are absorbed by the body relatively quickly. Similarly, we do not advise longer-acting fillers such as silicone, as the long-term risks are not currently known.
This foot type is characterised by a first metatarsal that is shorter than the others. The result is that the second, third and fourth metatarsals take more pressure, which leads to overload, metatarsal shear and, often, the formation of a neuroma.
In cases of Morton’s foot type, we will initially attempt to achieve normal loading across the metatarsals by non-surgical means, and treat the neuroma through techniques such as cryosurgery. Where symptoms persist, Mr McCulloch may offer surgery to correct the length of the metatarsals.
The nerve between the third and fourth toes may be anatomically thicker than the nerves between the other toes. This naturally-occurring thicker nerve may be at risk of developing a neuroma, especially if other risk factors, such as increased pronation, are present.
Sporting Causes
Some sports carry a higher risk of participants developing Morton's neuroma. As part of our sport-specific management, we routinely treat elite and professional athletes and we have consulted for several premiership football teams. Mr McCulloch was a Consultant at the 2012 Olympics.

Our experience and research shows that skiing is particularly associated with Morton's Neuroma. Some patients find that their symptoms only occur during skiing. This undoubtedly relates to the inflexible nature of ski boots (the condition is less common in snowboarding where the boots are softer).
Treatment for skiers involves reducing hypermobility of the foot by using lightweight orthoses and increasing the internal volume of the ski boot.

Road biking is particularly associated with Morton's neuroma. This is due to the often-narrow design of cycling shoes, elevated forefoot forces and the repetitive nature of the sport.
Our Centre will advise on which cycling shoe to obtain and we work closely with a number of excellent bike fitting companies.
We often recommend cycle-specific orthoses to manage a neuroma related by cycling.

Morton's neuroma is often more common in long-distance runners because of the repetitive nature of the sport, which accentuates small disturbances in forefoot pressure distribution.
We will provide the appropriate treatment after conducting in-depth gait analysis. This often involves changing footwear and includes selecting the right trainers for the particular type of foot and sport.

Footballers have a greater risk of developing Morton's neuroma. This is due to the high-impact nature of the sport and that fact that players often wear their boots relatively tight. Our Centre has successfully performed both open surgery and cryosurgery on professional footballers with Morton's neuroma.
Dance and golf are just some of the other sports that are more frequently associated with Morton's neuroma.
Treating athletes who suffer from Morton’s neuroma requires a sport-specific approach. For example, a ballet dancer will require dedicated medical appliances that are compatible with a ballet pump.
Footwear Causes
Shoes are a major cause of Morton's neuroma. Some patients experience minimal pain in the summer months due to being able to wear sandals, whilst others experience pain all year round.
Virtually all studies demonstrate a much higher incidence of Morton's neuroma in women (a ratio of 7:3). Footwear is likely to be a major contributing factor. That’s why we consider footwear advice as integral to managing the condition effectively.
The ideal footwear choice is often a wide shoe with a lace or strap, a slight heel and excellent forefoot cushioning. Any shoe that causes excessive side-to-side pressure can provoke issues. This is why skiers and cyclists suffer more frequently from Morton's neuroma.
Shoes that may help with Morton's neuroma:
Compression of the foot is a major aggravating cause of Morton's neuroma; we therefore do not recommend shoes with a narrow toe box. Shoes by Mephisto, Hotter and Clarks (e.g. Clarks Wave) often offer good support with a wide toe box.
We often recommend specialised trainers based on foot and sport type. The image to the left shows a typical shoe for runners with mild to moderate instability. This shoe is also suitable for casual use.
Our pressure studies have consistently shown increased forefoot pressures at the location of the neuroma. A thin-soled shoe (especially when combined with a high heel) significantly increases forefoot pressures. Wearers of these types of shoes are therefore at greater risk of developing a neuroma.

This kind of footwear has been shown to reduce symptoms in many patients. The benefits include a reasonable heel height, which reduces tension on the nerve, alongside a slight rocker effect and significant forefoot cushioning. In particular, FitFlop sandals reduce side compression on the foot. This is why some patients find the sandal version more helpful than the shoe version.

Completely flat shoes can aggravate Morton's neuroma in people who have tight calf muscles and reduced associated ankle flexibility. Individuals with good flexibility are often able to tolerate flat shoes and may suit a flat trainer like those by "Converse".

Some patients find these helpful.
Benign Joint Hypermobility
Benign joint hypermobility syndrome (BJHS) – or Ehler's Danlos type 3 – is a form of joint looseness that can have a negative impact on foot function.
BJHS is sometimes known as "double-jointedness", however this term is somewhat misleading. This particular syndrome is inherited and associated with a range of possible symptoms. If present in the foot, it tends to lead to reduced stability and abnormal pronation (excessive lowering of the arch and a collapsing ankle when the foot should be more stable during walking and running)
This causes the metatarsals to move too much, which leads to friction on the interdigital nerves and possible formation of a neuroma.
We have worked with world-renowned experts in the field of BJHS for many years, including Prof Rodney Grahame and Dr Alan Hakim. Mr McCulloch, the Centre's director, is a published author in the field of BJHS in associated with chronic pain –Hypermobility, Fibromyalgia and Chronic Pain 1st Edition.
In these cases the condition may not be diagnosed easily because most doctors do not test the foot when assessing for the condition.
At the Morton’s Neuroma Centre, we use a range of approaches to treat hypermobility. We generally take a combined approach after analysing the results of our in-depth gait investigations. This often includes physiotherapy and gait re-education, orthotic intervention, specialist footwear advice and a range of other possible interventions.
When treating a neuroma, the risk of complication increases in patients who have BJHS. We therefore generally recommend minimally-invasive treatments such as cryosurgery for people with this condition.